INTRODUCTION
Approximately 3400 infants die each year in the U.S. from sleep-related deaths. Not only are sleep-related deaths a leading cause of infant deaths, the elevated death rate from sleep-related causes has persisted for the last 20 years (Centers for Disease Control and Prevention 2020). Furthermore, as with many non-communicable and preventable adverse health conditions and outcomes, there also are large racial, ethnic, and socioeconomic disparities associated with sleep-related infant deaths.
Sleep-related deaths include deaths classified as a Sudden Unexpected Infant Death (SUID), defined as the unexpected death of an infant in which the cause of death was not obvious prior to investigation. SUID encompasses Sudden Infant Death Syndrome (SIDS), accidental suffocation or strangulation of an infant during sleep, and deaths from an undetermined cause (Centers for Disease Control and Prevention 2024).
In 2019 in Cook County, Illinois, which includes the city of Chicago, 91% of infants who died unexpectedly had sleep-related causes noted on their death certificates (Illinois Violent Death Reporting System 2010). In Cook County in 2020, SUID was 16 more times likely to occur in non-Hispanic Black infants, and four times more likely to occur in Hispanic infants when compared with non-Hispanic White infants (Illinois Department of Public Health 2020). In addition, a study by Briker et al. (2019) showed that nearly 30% of sleep-related infant deaths in Cook County occurred in a residence that was not their own, which raised awareness that infants are being cared for by a range of caregivers outside of their own homes but also further complicated potential approaches to address this issue within communities.
The basic principles of infant safe sleep, such as placing an infant on their back and lying an infant on a firm surface and in their own bed, are often shared with families in the clinical setting by health care professionals at regular well-child visits. However, recent data shows that many caregivers may not be aware of these basic principles, since in one study of Chicago parents only 70% reported receiving safe sleep advice from their doctor or nurse (Rush University Medical Center 2023). Other common sources where parents have reported learning about infant safe sleep have included family members (58%), social media/blogs/websites (30%), and friends or neighbors (22%) (Rush University Medical Center 2023).
There are a range of reasons why accurate information about safe sleep practices may not be effectively conveyed in the health care setting or understood by caregivers. For one, primary care providers often have limited time during well child visits to have in-depth discussions with families about topics other than the reasons for their visits. In addition, medical advice, such as anticipatory guidance regarding safe sleep practices, can come across as paternalistic or culturally insensitive if a provider has yet to develop a trusting relationship with a family or to understand what communication style is most effective for a family (Willems et al. 2005).
An effective and growing method for sharing important health information is through community health workers (CHW). One successful model for community member involvement in healthcare exists in Chiapas, Mexico through Compañeros En Salud (CES). CES trains Acompañantes, which translates to ‘companion’ in English and is commensurate with the role of CHW in the U.S., to provide basic health education and management for diabetes and hypertension in remote rural communities that have limited access to physicians (Partners in Health 2012). By utilizing companions or trusted community members to provide needed medical management and counseling, this model has found success and improved health in the community.
In recognition of these combined factors: SUID has not declined in over two decades; minoritized infants are disproportionately impacted by sleep-related deaths; health care providers have limited time and may not be seen as a trusted source of safe sleep advice; and many infants die from sleep-related deaths in homes that are not their own, our project team was driven to develop and pilot an intervention to train community members to become Safe Sleep Ambassadors (SSA).
Taking inspiration from the CES model, the project team hypothesized that training trusted community members to become SSA and provide information to caregivers about proper infant safe sleep practices would improve safe sleep adherence in communities where lack of trust in health care workers may serve as a barrier to implementing safe sleep practices. Further, recruiting and training community members who reside in the South and West side neighborhoods of Chicago would be essential to reach families who reside there, and would result in an increase in the number of informed infant caregivers in the communities identified as being the most impacted by SUID (Mason 2017). The study team also aimed to determine if the SSA model is a feasible and effective strategy to reinforce the importance and practice of infant safe sleep among infant caregivers in targeted Chicago communities, which may improve implementation of and adherence to safe sleep practices and help reverse the course of decades of sleep-related deaths.
METHODS
Project Team
The project team was led by staff of the Injury Prevention and Research Center (“Injury Prevention and Research Center,” n.d.) based at Ann & Robert H. Lurie Children’s Hospital of Chicago and included a medical student and faculty mentor.
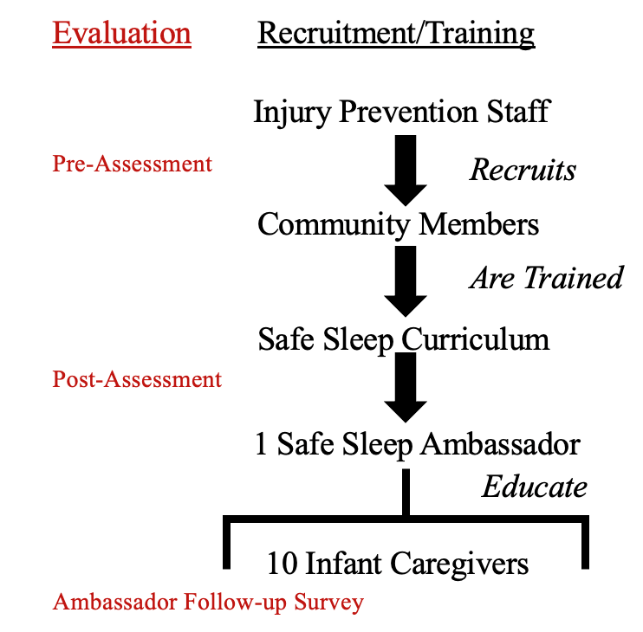
A conceptual model for training and evaluating the SSA program is provided in Figure 1. The training process progresses from recruiting participants, to training them using a safe sleep curriculum, and preparing them to become SSA who can educate infant caregivers living in their own communities to model safe sleep practices. The evaluation components of the study are included on the left side of the figure and are described in detail below.
The Institutional Review Board of Ann & Robert H. Lurie Children’s Hospital of Chicago determined this study to be exempt from ongoing oversight as it involved no greater than minimal risk to participants.
Safe Sleep Ambassadors
Recruitment
Starting in 2020, South and West side community members were recruited to be SSA. Recruitment occurred through referrals from organizations located in those communities including the Women, Infants, and Children (WIC) office and community partners. There were no demographic restrictions to participation.

Training
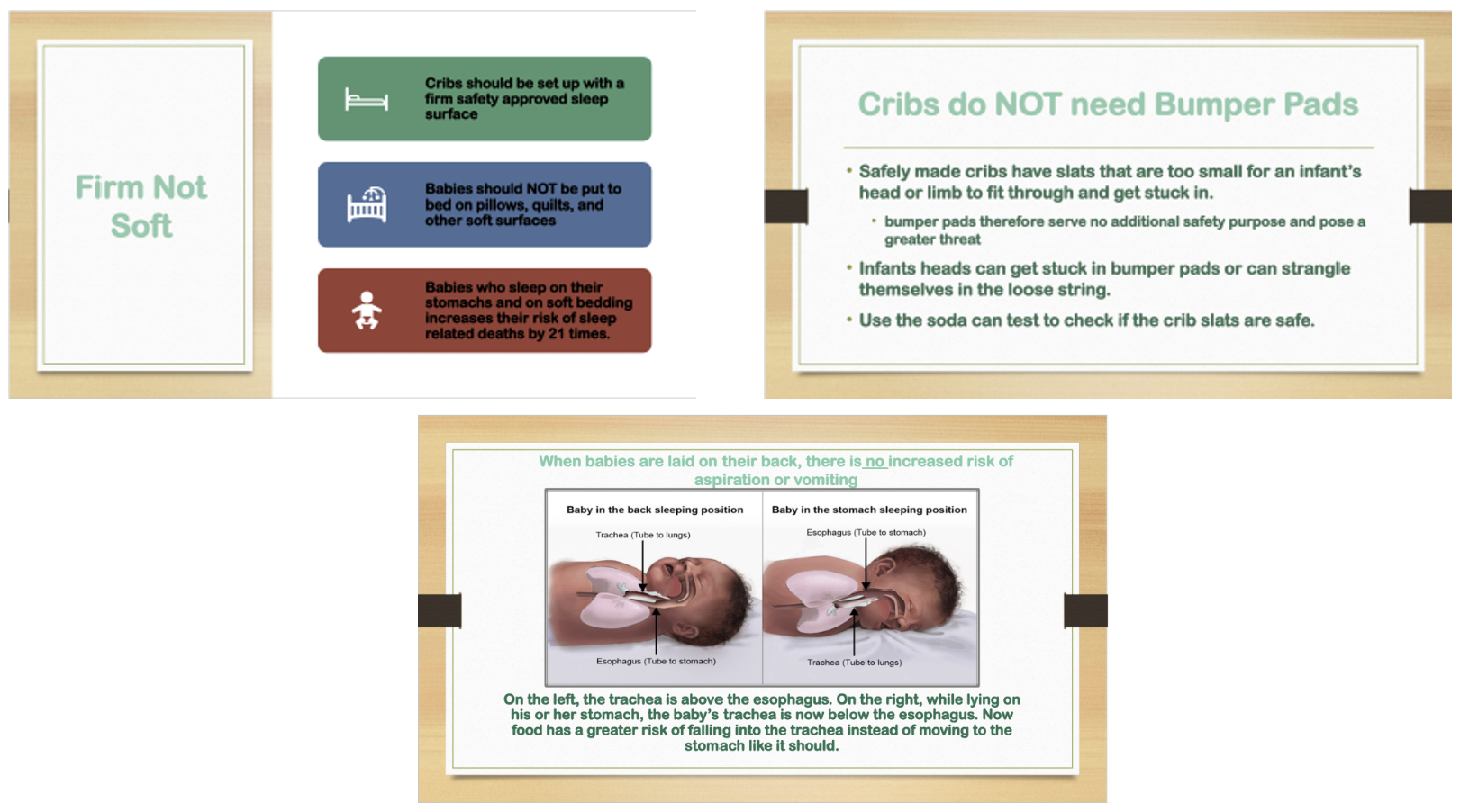
Participants attended ~ 1-hour training sessions conducted by injury prevention center staff over Zoom. The training followed a safe sleep curriculum developed by staff and based on safe sleep principles promoted by organizations that champion infant safe sleep including the National Institutes of Health (NIH), Cribs for Kids (Cribs for Kids 2022), and the National Institute for Children’s Health Quality (NICHQ) (Figure 2). NICHQ is an organization committed to achieving better health outcomes for children through lasting system changes and advocating for promoting a safe sleep culture by first building “foundations of trust” within underserved areas (NICHQ 2022).

Pre- and Post-Training Knowledge Assessments
Prior to the SSA training, participants completed a five-question pre-assessment survey to ascertain their knowledge of key elements of infant safe sleep practices. Following the training, a post-assessment survey was administered, which replicated the questions of the pre-assessment and included two additional questions regarding the effectiveness of the training (Table 1).
Assessments included questions that are essential to an understanding of safe sleep and reflect material addressed in the safe sleep curriculum. Responses to the assessment questions were allotted a point value (range from 1 to 3; total scores ranged from 0 to 10) to be able to compare findings qualitatively and quantitatively across assessments. A follow-up survey was administered one year after the SSA training to better understand the demographics of the community members trained by the SSA, and to collect other information the SSA wanted to share about the process and their experiences. At the completion of training, SSA were given a gift card ($150) for their participation.
All trainings and assessments were conducted in English. Surveys were distributed anonymously through Qualtrics and analyzed qualitatively and quantitatively. Paired T-tests were used to analyze changes in knowledge scores for individual responses.
Ambassador-led Safe Sleep Information Sessions
After completing the training, SSA were instructed to identify and reach out to individuals they knew who were involved in infant care, and to deliver safe sleep information sessions to 10 individuals within their own social networks who live in their community. Each SSA was provided with 10 safe sleep kits to distribute at the information sessions. Safe sleep kits contain items approved by the American Academy of Pediatrics (AAP) for infant safe sleep including a sleep sack, a “Sleep Baby Safe and Snug” book by Dr. John Hutton (Hutton and Busch 2013), a pacifier, and additional safe sleep information produced by Ann & Robert H. Lurie Children’s Hospital of Chicago based on information developed by the AAP.
RESULTS
A total of 22 community members were recruited and trained to be SSA during the two-year pilot project period from 2020-2021 (Table 2). Of the 22 SSA, 11 were mothers and 1 father, 7 were nursing students, and 3 were volunteer professional staff at community-based agencies—all of whom resided in a South or West side Chicago community. The majority of those recruited and trained to be SSA were mothers who were associated with a local community-based organization that works to improve the health and well-being of Chicago youth living in disinvested communities.
Program Evaluation
Assessments
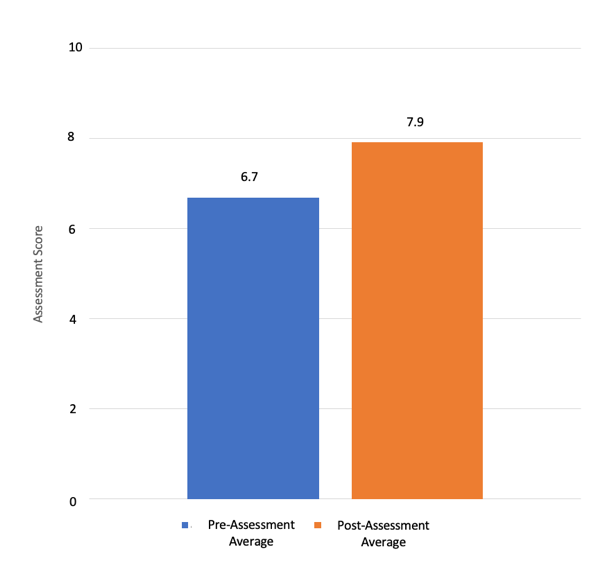
All 22 SSA completed the pre-assessment and 12 completed the post-assessment. The mean knowledge score on the pre-assessment was 6.8/10 (range: 4 to 9). Of the 12 individuals who completed the post-assessment, the mean knowledge score increased from 6.7 to 7.9. The overall knowledge change among individuals who completed both the pre- and post-assessments was found to be significant in a paired-means t-test (p = 0.03, Figure 2).

In response to Assessment Question 3: List three things that are protective against Sudden Unexpected Infant Death (correct answers were breastfeeding, pacifier use, and smoking avoidance), individuals most often missed breastfeeding and pacifier use in their response.
Qualitative changes in the content of the open-ended responses from the pre-assessment to the post-assessment were also compared. It was noted that responses became more accurate and more thorough following the training, moving from a general to a more specific response and from a limited understanding to a broader understanding of safe sleep practices. For example, a pre-assessment response to the question, What have you been told about keeping infants safe while they sleep? was, “I know that they should be on their backs” while the post-assessment response became “…that when a baby lies on their back it.. reduces the risk of choking… in this position the trachea is above the esophagus.” Additional example responses to Assessment Question 1 are provided in Table 3. Comments from SSA on the post-assessment regarding their perspectives about the information provided during the training included, " I liked the resources that were provided. Especially since they are in Spanish" and “the presentation was clear and concise with about the right amount of information on the topic.”
Safe Sleep Ambassador Caregiver Training Outcomes
SSA reported educating a total of 96 community members and distributing 96 kits to mothers, fathers, aunts and uncles, and grandparents. Among the 22 SSA trained, 6 reported successfully conducting 10 training sessions each and distributing all 10 of their respective safe sleep kits. In addition, study staff reported that several SSAs asked for additional safe sleep kits and were inspired to continue reaching out to more infant caregivers in their community, which suggests that several SSA likely completed over 10 trainings. Ambassadors primarily reported that they reached out to friends and families in their social networks but were also referred to additional caregivers. In general, the cohort of nursing students trained to be SSA was less successful in identifying caregivers and conducting training sessions.
In the one-year follow-up surveys with the SSA, the following comments were provided when asked about the project in general: “I think that this was an awesome project because most parents are not aware that they are putting their babies at risk just by the way they put them down for bed or even for a nap!” and “The gift bags helped people stop and listen.” Additionally when asked how they could be better supported, SSA reported: “I was already well equipped” and “There was adequate support and training.”
DISCUSSION
This pilot study of the Safe Sleep Ambassadors (SSA) program demonstrated that it is feasible to recruit and train community members to educate infant caregivers in a community setting about infant safe sleep practices. After a short training session, SSA reported delivering the infant safe sleep education and distributing the safe sleep kits, which contained items to reinforce the safe sleep education.
Designed to model the Compañeros En Salud community health worker model (Partners in Health 2012) employed in Chiapas, Mexico, the SSA project focuses on the advantages of gaining knowledge provided by fellow community members. We know that there are many other sources of information about infant sleep outside of medical advice that are available to parents including family members, social media/blogs/websites, and friends or neighbors. Our growing awareness about where contradictory information comes from helps us to know how best to address misconceptions and distrust through training SSAs and responding to feedback from infant caregivers in Chicago communities. SSA can replace inaccurate information and instill trust. As more caregivers attend SSA trainings, more family members, friends, and neighbors—all of whom serve as caregivers in these communities—will have access to accurate sources of information about infant safe sleep.
Ambassadors with the most effective outreach—those who reported conducting at least 10 training sessions—were individuals with established relationships with local community-based organizations and thus were better able to identify individuals who would benefit from the training sessions. As noted, SSA who could not rely on their social networks within the community lacked comradery and experienced more challenges identifying individuals with whom to conduct trainings. To address this gap and support more individuals who want to serve as SSA, future trainings should include additional resources along with facilitated connections to community leaders to help identify infant caregivers in those communities.
It is not surprising that the SSA model was most successful when well connected, trusted individuals within their respective communities shared health information. Based on this outcome, we hypothesize that when the individual providing the information is trusted, the information shared is more likely to be trusted and applied. To test this hypothesis, future trainings should include follow-up surveys with caregivers who participated in the training sessions to learn if and how they implemented what they learned and to gather their questions and insights about how to improve the program. To increase the number of trainings by SSA, we are considering developing a certificate system and providing other benefits to SSA as well as establishing a more effective way for SSA to track completed trainings and report back in real time to aid in improving subsequent trainings.
When evaluating the training components, while safe sleep knowledge scores were high at baseline, there was a statistically significant increase in knowledge after the training session. However, because not all questions were answered correctly or completely in the post-assessments, we have since modified the training to expand on and more clearly address the topics covered by the assessment questions. As the safe infant sleep information continues to be disseminated in these Chicago communities, we expect that even pre-assessment scores will be higher among future participants, which may also present a way to evaluate the spread of this important health information. Informed by the findings of this pilot project, we have expanded our efforts by hiring a full-time staff member to train additional SSA who in turn can educate more infant caregivers in the communities where sleep-related deaths occur most.
Beyond the study outcomes, during the evaluation process the project team recognized and reflected on other key aspects of the SSA program that may have helped lead to its success. First, due to their previous experience working in the West and South Side communities, the project team knew what safety messages would resonate best with community members. For example, it is common for caregivers to worry that “a baby will choke if they are placed on their back.” However, this concern can be allayed by showing simple anatomy drawings of the “windpipe” and “food tube” that demonstrate that babies are safer when the “windpipe” is on the top of the “food tube” which occurs when a baby is placed on their back. While the safe sleep training curriculum is supported by high quality science, knowing how to fine tune the training to anticipate and address community member and caregiver concerns is essential and leads to increased trust.
The training also included discussions about the fact that the title “infant caregiver” extends beyond mothers and fathers, which is why SSA were encouraged to reach out to and train aunts, uncles, and grandparents. Recognizing the importance of expanding this definition by involving more individuals who care for infants and children, possibly in their own home environments, may be an additional strategy to decrease the incidence of SUID, particularly in high-risk communities.
This study did have several limitations that should be noted. First, it was not possible to know for sure if the participants conducted the trainings, how many people they trained, or what information was shared during the trainings. However, we believe the participants to be trustworthy and motivated to do the trainings, and feedback from SSA also suggest that the information they shared was accurate. We also experienced several limitations during the implementation of this project. Due to constraints related to the COVID-19 pandemic, the process of recruiting and training community members to be SSA was delayed and then redesigned to be a virtual training only. Additionally, SSA voiced challenges engaging with community members during the COVID-19 pandemic. While this was a particularly challenging time for everyone, we do not expect to experience this level of issues in future trainings.
Additional data that was not collected would have been helpful to further understand the implementation and outcomes of the SSA training and outreach efforts. For example, we did not require participants to complete the post-assessments, which contributed to the lack of post-assessment responses. In addition, creating a more intentional space for SSA to share what they learned during training sessions with caregivers could have helped strengthen the culturally-tailored educational messages. We aim to build these elements into future trainings. Future studies should also consider assessing the teaching skill of the SSA, not just knowledge change. In addition, it will be important to assess if caregivers trained by the SSA applied their new knowledge about infant safe sleep practices through creating safer sleep environments in their homes.
While SUID rates have remained essentially unchanged for over two decades, this pilot project showed the promise of engaging and training community members to serve as trusted safe sleep ambassadors in communities disproportionately impacted by SUID. While the results of this pilot study provided initial data to show proof-of-concept of the SSA program, additional studies will be needed to further assess the training process and measure the impact of this community-engaged educational intervention.
We hope that learning about our work to improve safe sleep practices in Chicago communities inspires others to start similar programs, with the goal of reducing sleep-related deaths across the U.S. and beyond.
Acknowledgements
We extend a special thanks to all the Safe Sleep Ambassadors for participating in this pilot project and reaching out to their contacts to educate caregivers about safe sleep practices. We are grateful to the entire staff of the Injury Prevention & Research Center at Ann & Robert H. Lurie Children’s Hospital of Chicago for partnering with us, and the Patrick M. Magoon Institute for Healthy Communities for supporting our efforts to reduce rates of SUID in Chicago.
Funding/Support
Funding for this project was provided through the Patrick M. Magoon Institute for Healthy Communities.
Declaration of Competing Interests
The authors of this paper have no competing interests or relevant disclosures to declare.
Author Contributions
KS and MD conceptualized and designed the study and conducted data analysis; AH trained the study participants and collected data; MD designed the training materials and surveys and drafted the manuscript; KS, AH and MD edited the final manuscript for submission and take full responsibility for its content.