
INTRODUCTION
Through the delivery of clinical care, physicians routinely advocate for the needs of individual patients by helping them access needed resources or arranging appropriate and timely treatment. But physicians’ role as health advocates does and should encompass multiple levels, including engaging in system- and population-level advocacy, which is essential to influence the structural and social determinants of health and health inequities that adversely impact their patients and society on a broader scale (Fried, Shipman, and Sessums 2019; M. A. Earnest, Wong, and Federico 2010).
Among many internal medicine (IM) trainees, physicians, and professional organizations, population-level advocacy is viewed as a professional obligation (Gruen, Campbell, and Blumenthal 2006; DeGrazia, Ogunwole, Pollack, et al. 2022; ABIM Foundation, ACP-ASIM Foundation, and European Federation of Internal Medicine 2003). For example, in “The Physician’s Charter,” the American Board of Internal Medicine (ABIM) Foundation and American College of Physicians (ACP) endorse population-level advocacy as a key strategy for achieving the profession’s commitment to social justice (ABIM Foundation, ACP-ASIM Foundation, and European Federation of Internal Medicine 2003). This view of advocacy also informs accreditation standards for Accreditation Council for Graduate Medical Education (ACGME) common program requirements, which assert that resident physicians in all specialties must demonstrate not only competence in advocacy for quality patient care and optimal patient care systems but responsiveness to the larger context and system of health care, including the structural and social determinants of health, and an ability to incorporate considerations of equity at the population level (Accreditation Council for Graduate Medical Education, n.d.-b, n.d.-a).
Despite IM physicians’ views about the importance of advocacy and ACGME program requirements addressing advocacy, our prior study of existing advocacy curricula in U.S.-based IM residency programs showed that fewer than half of IM residencies offer formal population-level advocacy curricula (Burnett, De Lima, Henry, et al. 2024). To help IM residencies without population-level advocacy curricula identify curricular needs and develop population-level advocacy curricula, we surveyed program directors (PDs) of IM residency programs without existing advocacy curricula. Our aims were to 1) identify whether IM residency programs without population-level advocacy curricula were planning such curricula; 2) characterize planned curricula; and 3) identify barriers to implementing population-level advocacy training. Gathering and sharing these data can help IM programs identify curricular needs and develop advocacy curricula to train the next generation of population-level health advocates.
METHODS
The Association of Program Directors in Internal Medicine (APDIM) conducts an annual multi-themed, nationally-representative survey of IM residency PDs. PDs were selected as respondents as they are recognized as the most appropriate faculty leaders to provide representative data on IM education and training. The annual APDIM survey contains questions that identify best practices, help PDs advocate for resources, address topics of interest to the graduate medical education (GME) community, and inform resident educational policies and program strategic planning. The 2022 APDIM survey also contained a section of questions on population-level advocacy curricula in IM programs, including whether an IM program had an advocacy curriculum or planned to develop one; however, planning was not specifically defined in the survey. A detailed description of the study methods including study design, setting, participants, survey development, and data collection was published previously and includes access to the full 2022 APDIM survey (Burnett, De Lima, Henry, et al. 2024). Following Earnest et al., for the purpose of the survey, we defined advocacy as “action by a physician to promote social, economic, educational, and political changes that ameliorate the suffering and threats to human health and well-being.” (M. A. Earnest, Wong, and Federico 2010) In addition, we specified that the focus of these survey questions was population-level advocacy.
Briefly, the 2022 survey was sent to all 456 APDIM member programs, which represented 80.0% (456/571) of all U.S.-based IM residencies with ACGME accreditation. Programs were excluded if they did not have “initial” or “continued” ACGME accreditation status prior to the most recently completed academic year or if they did not fill any IM residency positions as of the most recently completed academic year. These criteria ensured that all survey respondents would be capable of providing representative responses. In this context, programs with “initial” ACGME accreditation were new programs that were determined to meet ACGME Internal Medicine Review Committee accreditation requirements within the past two to three years.
PDs who indicated that their IM residency program did not include an advocacy curriculum but reported planning to develop one were asked how they would structure it and what they would teach (Table 1). To answer the questions, respondents selected predetermined options that included “Other,” which prompted a free-text field. Those without a current advocacy curriculum were also asked about perceived barriers to implementing one and the perceived importance of a population-level advocacy curriculum by their IM program leadership, IM residents, and overall institution. Again, respondents selected from pre-determined options. After pilot testing the survey among the APDIM Survey Committee, which consisted of 12 physician members with experience as IM PDs or associate PDs, the online APDIM survey was deployed by email on August 16, 2022 and closed on December 13, 2022. Email reminders were sent up to six times. The study (#22-AAIM-117) was deemed to be of no greater than minimal risk to participants and therefore exempt from full Institutional Review Board (IRB) review by Pearl IRB (U.S. DHHS OHRP #IRB00007772), an independent review board fully accredited by the Association for the Accreditation of Human Research Protection Program Inc.
Statistical analysis was conducted in Stata 16.1 SE (StataCorp), SPSS version 29 and R version 4.1.3. Descriptive statistics were used to assess the prevalence, scope, structure, and content of planned advocacy curricula. Adjusted Wald (Pearson) Chi-square tests were used to assess categorical variables, and nonparametric (equality-of-medians) tests were used to assess continuous variables. All tests were two-tailed. Alpha was set at 0.05 for determining statistical significance. To assess the statistical representativeness of the results, we compared the program characteristics of those who responded to the survey to the total population surveyed. To achieve this, prior to de-identifying the final responses, the study dataset was appended with residency program data using external sources, including the U.S. Census Bureau for geographic regions, ACGME Accreditation Database System (Public) online, and with similar data from the American Medical Association (AMA) and ABIM.
RESULTS
Of 456 survey-eligible programs, 276 (61.0%) PDs completed the survey. No statistically significant differences were found between respondents and non-respondents, based on key characteristics that defined the survey population (Table 2). Out of 276 respondents, 148 (53.6%) reported not having a current population-level advocacy curriculum. Thirty-three (22.3%) of those with no population-level advocacy curricula reported actively planning for one. When specifically examining how closely the IM programs without a population-level advocacy curriculum represented the complete survey population, we found no differences across most key residency program characteristics, including program type (e.g., community-based, university-based, etc.), program region (e.g., Midwest, Northeast, etc.), and program size (i.e., number of ACGME approved residency positions) (Table 2). The only statistically significant difference noted was that programs with initial ACGME accreditation were more likely to report planning for a population-level advocacy curriculum compared to programs with continued accreditation (18.2% vs 3.5%, p=0.01).
Curricular plans for population-level advocacy content and instructional methods varied (Figure 1). The most frequently reported planned methods of instruction included didactics (64%), experiential learning (51%), and advocacy projects (43%). The most frequently reported planned topics were foundational concepts of physician advocacy (e.g., definitions, professional code of ethics, general principles, social determinants of health) (74%) and health policy (64%); community organizing and legislative advocacy, which more directly reflect population-level advocacy, were reported at 36% and 27%, respectively.

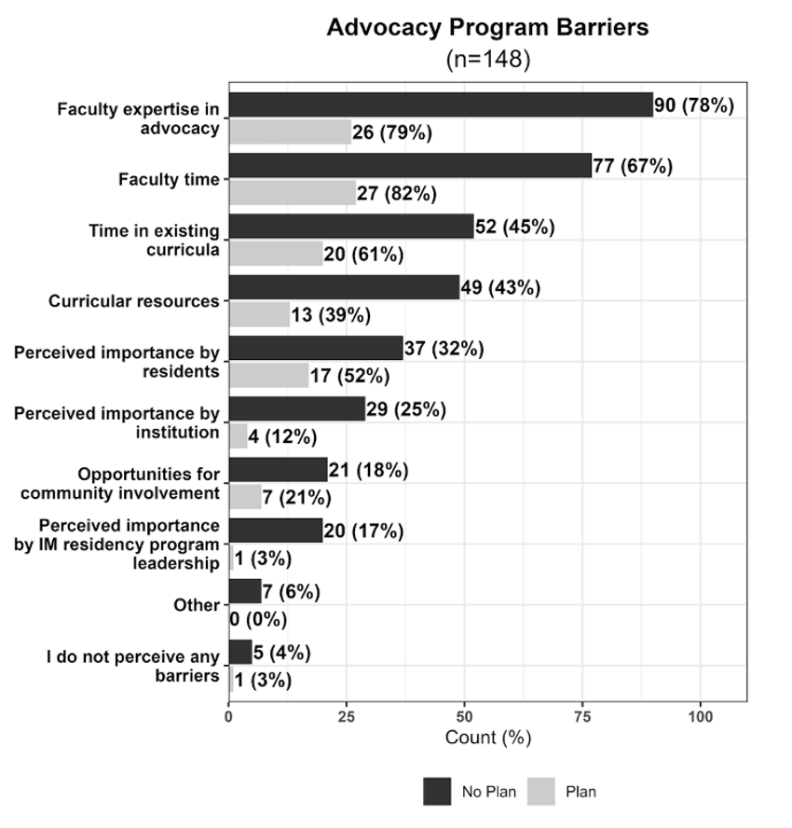
Commonly reported barriers to teaching a population-level advocacy curriculum, which included lack of faculty expertise, faculty time, and time in existing curriculum, were comparable between programs that were planning for a curriculum and those that were not (Figure 2). Additional barriers among non-planners, which were noted via free-text response, included lack of funding, affiliation with military training institutions, and conflict regarding what physicians were permitted to do in public forums.

DISCUSSION
In this national study of IM residency programs, we found that among IM programs without an advocacy curriculum, most (>75%) were not planning to offer a population-level advocacy curriculum. Curriculum planners reported a variety of planned curricular content and methods, which correspond with the content and methods used by IM programs that currently offer population-level advocacy curricula, as reported in our previous study (Burnett, De Lima, Henry, et al. 2024).
Importance of Advocacy Training to and for IM Residents
Although more than 90% of IM physicians describe population-level advocacy as important, fewer than half of IM residency programs currently provide advocacy training (Gruen, Campbell, and Blumenthal 2006; Burnett, De Lima, Henry, et al. 2024). The findings from this study provide further evidence that among U.S.-based, IM residency programs without a current curriculum, few are planning to offer one. To better understand the context in which this occurs, comparisons across medical specialties offer some key insights into the relative absence of population-level advocacy curricula in IM residency programs.
ACGME common program requirements for all medical specialties state that resident physicians must demonstrate competence in advocacy, responsiveness to social determinants of health, and an ability to incorporate considerations of equity at the population level (Accreditation Council for Graduate Medical Education, n.d.-b, n.d.-a). However, published curricula addressing population-level advocacy are—with the exception of specialties oriented toward primary care, especially pediatrics—uncommon in GME literature (Howell et al. 2019). Among specialties where cross-sectional studies of advocacy training exist, studies from 2020 showed that only 37% of family medicine programs required population-level advocacy training for all residents, whereas only 7 of 236 (3%) psychiatry programs provided any population-level advocacy training (Accreditation Council for Graduate Medical Education, n.d.-a; Coutinho, Nguyen, Moreno, et al. 2020; Vance and Kennedy 2020). One possible explanation for the low rates of formal population-level advocacy curricula in those specialties is that ACGME common program requirements regarding advocacy are not entirely well-defined and may have been misinterpreted. If programs leaders interpreted the advocacy competency requirement to apply only at the level of individual patients in the course of clinical care, they may have overlooked the intended emphasis on population-level advocacy. This may also explain the lower rates of planning for a population-level advocacy curriculum among IM residency programs without one in our study.
In contrast, more than 90% of pediatrics residency programs reportedly teach population-level advocacy skills (Lichtenstein, Hoffman, and Moon 2017). Two factors that do not exist for other specialties are thought to explain the higher rate of advocacy training in pediatric residency programs. First, the ACGME Pediatrics Resident Review Committee created explicit expectations for population-level advocacy training, suggesting that clarifying the meaning of ACGME training expectations may be an important impetus for advocacy curricular growth and standardization across specialties in GME (Fried, Shipman, and Sessums 2019; Burnett, De Lima, Henry, et al. 2024). Second, the American Academy of Pediatrics directly supports residency programs to develop and implement advocacy curricula in pediatric residency programs (Burnett, De Lima, Henry, et al. 2024; Howell et al. 2019). Although the absence of these factors in IM may explain the lower rate of population-level advocacy curricula offered in IM compared to pediatrics, it does not explain why some IM programs are planning advocacy curricula while others are not. Further, although the 2022 APDIM survey did not ask PDs about why they were or were not planning to offer a curriculum, it is noteworthy that some programs were planning curricula despite facing significant barriers. One possible explanation is that PDs felt it was important to teach population-level advocacy to IM residents. Consistent with this interpretation of the results, among programs planning curricula, only one PD reported low perceived importance by IM program leadership.
Barriers to Providing a Population-level Advocacy Curriculum in IM
Our findings on the barriers to providing a population-level advocacy curriculum in IM programs without a current advocacy curriculum suggest that both those planning a curriculum and those not planning one face the same primary barriers—lack of faculty expertise, faculty time, and time in existing curriculum.
Lack of faculty expertise in advocacy was the most commonly reported barrier for both curriculum planners and non-planners and was as much a barrier for planners as it was for non-planners. The finding regarding a lack of faculty expertise suggests that formal faculty development in population-level advocacy may be an important strategy for promoting faculty expertise—however, who will provide it? As Winthrop and colleagues note, whether the source is formal training or personal experience, faculty need baseline knowledge, appropriate language, and related tools to effectively teach advocacy and to advocate for and create population-level change (Winthrop, Michelson, and Nash 2021). To achieve this, some IM programs may wish to explore partnerships with faculty in other specialties (e.g., pediatrics), staff in their institution’s government affairs offices, members of local medical professional societies, or community organizations and activists to serve as expert guest lecturers in resident curricula. Partnerships with these groups can also expand the expertise of current faculty through faculty-focused advocacy training. Alternatively, IM faculty may consider participating in external faculty development programs in advocacy and health policy, such as the Society of General Internal Medicine (SGIM)'s Leadership in Health Policy (LEAHP) program (Kyanko et al. 2022).
Unexpectedly, lack of faculty time and lack of time in existing curricula were reported more commonly by curriculum planners than by non-planners. It is possible that being in the process of planning for an advocacy curriculum increased planners’ awareness of what is needed and what they do not possess; at the same time, 4% of non-planners reported no barriers to having an advocacy curriculum. The finding that faculty time is a common barrier to implementing a population-level advocacy curriculum suggests that IM faculty and programs may lack protected time and support for teaching advocacy, which is not surprising since these are commonly reported barriers to adding virtually any new content to medical curricula. Specific to advocacy education, one hypothesis for the lack of support for teaching advocacy in IM residencies is that a culture of community- or population-level advocacy is uncommon in IM departments and therefore the time and effort needed to teach advocacy is not recognized. Another hypothesis is that teaching advocacy curricula may be assumed to fall on faculty with interests in related topics such as social determinants of health, health equity, and anti-racism, for example. As many faculty working in these spaces already feel insufficiently supported in their work, PDs may assume (correctly, in many cases) that these faculty lack the time to add even more to their workload (Raphael et al. 2023). Regardless of the reasons, supporting faculty with time and resources is key to training residents to become physician-advocates (Nerlinger and Shah 2022). Thus, further research will be needed to better understand the specific reasons for why population-level advocacy education is not offered more and how it can be better supported in IM departments and IM residency programs.
Among common barriers, the finding that residency programs lacked time in existing resident curricula suggests that some methods of teaching advocacy curricula may be particularly challenging to implement. For example, experiential learning often requires additional resources including time, funding, and access to diverse patient populations and community organizations (Burnett, De Lima, Henry, et al. 2024). When such resources are limited, experiential learning may not be feasible for all learners. This may explain why didactics were reported almost twice as much as experiential learning among programs planning population-level advocacy curricula. Although potentially more challenging and resource-intensive to implement, the benefits of teaching advocacy through experiential learning are well established: trainees value advocacy training through experience, and direct experience in advocacy is associated with greater competence and engagement in advocacy after completion of residency training (McDonald et al. 2019; Law et al. 2016; LaDonna et al. 2021). Further research is needed to understand both the barriers and facilitators of experiential learning for teaching population-level advocacy in IM residency programs.
Finally, the finding that access to curricular resources was a common barrier aligns with lack of expertise and time since both would be needed to develop appropriate resources. To address this gap, educators of IM residents may consider drawing from resources developed for undergraduate medical learners or GME learners from other specialties, including teaching and assessment tools, or drawing from issue-specific resources highly relevant to IM physicians and their patients, such as toolkits for advocacy on access to care, climate change and health, firearm injury prevention, and reproductive health (Hoffman, Rose, Ayoub-Rodriguez, et al. 2017; Sheehan, Bartell, Mangold, et al. 2023; Doobay-Persaud, Adler, Sheehan, et al. 2019; American College of Physicians, n.d.). The barriers reported by PDs, which represent both technical and adaptive barriers, are difficult but essential to overcome to provide an effective population-level advocacy curriculum. To do so, it also will be important to better understand how IM programs with current population-level advocacy training have achieved it and how IM programs who reported planning to offer such curricula overcome these barriers, as well as the impact on quality and outcomes of their training as reflected in resident assessments.
Drivers and Facilitators of Population-level Advocacy Curricula in IM
In assessing the factors driving some IM programs to plan for population-level advocacy curricula, although the survey did not directly ask about drivers or facilitators, presumably a primary driver is the importance of developing population-level advocacy skills. PD and/or faculty interest in advocacy may be driving curriculum planning in some IM programs. Although the group size was small, non-planners in our study reported the perceived importance of advocacy by IM program leadership and sponsoring institutions as a barrier much more so than curriculum planners. Similarly, interest in advocacy from prospective residents may be a driver of curriculum planning. Student interest in population-level advocacy is well established (Chimonas, Mamoor, Korenstein, et al. 2021; Simpson and Jarshaw 2022; Schreidah, Robinson, Tinsley, et al. 2024; Clarke 2024). Some IM programs thus may be evolving to recruit trainees who value population-level advocacy training.
Another possible facilitator of curriculum planning suggested by our results is initial ACGME accreditation status. This hypothesis is driven by the finding that programs with initial ACGME accreditation were more likely to report planning an advocacy curriculum compared to programs with continuing accreditation. This may suggest that implementing a new curriculum is easier when nothing prior existed, allowing more space for a new curriculum. However, these results must be interpreted with caution given the small number of programs in our study with initial accreditation. As interest in population-level advocacy grows, newer faculty at newer programs may also be more likely to have had some advocacy training and experience as compared to faculty at established programs who may not have had the same level of prior training or experience. Future surveys should assess how accreditation status factors into decisions to provide population-level advocacy programs and content. Further research is also needed to identify unique drivers and facilitators among programs currently planning to offer an advocacy curriculum, as well as how they are able to overcome reported barriers to implement an effective population-level advocacy program in IM and other specialties.
Suggestions for Implementing an Advocacy Curriculum in IM: The Need for Advocacy
Among IM residency programs planning curricula in population-level advocacy, some PDs expressed uncertainty about the methods and topics they plan to include in their curricula. This may suggest that some IM residency programs need guidance on how to develop effective population-level advocacy training. Although there is a lack of consensus on how to best teach advocacy, fortunately some evidence-based best practices have emerged in advocacy education, and a variety of curricular resources are now available (Hubinette et al. 2017). Here, we propose some methods and topics for advocacy education for IM residencies based on some reported best practices and available resources.
As mentioned above, research shows that experiential learning is likely the most effective method of instruction in advocacy education (McDonald et al. 2019; Law et al. 2016; LaDonna et al. 2021). Indeed, experiential learning is both effective and common. A recent systematic review of published advocacy curricula in GME programs identified that most programs included partnerships with community organizations and community-based advocacy projects as core experiential educational components (Howell et al. 2019). As lack of opportunities for community involvement was not frequently reported as a barrier in our study, IM programs should consider partnering with community organizations to develop and implement community-based advocacy projects. Importantly, when adopting community-based approaches, residency programs must ensure that the voices of community partners are elevated in these relationships. Hoffman and colleagues published curricular resources for teaching a practical approach to community-based advocacy that emphasizes advocacy with as opposed to advocacy for communities, which is a key element of population-level advocacy training and would reinforce the need for advocacy to focus on community needs (Hoffman, Rose, Ayoub-Rodriguez, et al. 2017). This flexible framework can be employed as a theoretical exercise or as a roadmap to create real-world change, enabling IM residency programs to adapt advocacy teaching to available resources. For example, in settings where programs face substantial barriers, the framework might be used to support residents’ self-guided learning. In settings where faculty time and community organizations are more abundant, the framework might be used to forge meaningful, faculty-facilitated community partnerships, which could not only be more effective than having faculty lead advocacy training (especially when their experience and time are limited) but could also lead to even more impactful advocacy.
No national consensus exists regarding the content of advocacy training or how to assess it, though it is still required by ACGME for accreditation. However, expert opinion and theoretical models suggest training topics should include both community and legislative domains to prepare residents for competence in population-level advocacy. In a modified Delphi study of physician-advocates, a group of experts in pediatric advocacy concluded that resident advocacy skill objectives at the community level should include, for example, developing relationships with those in need in the community and planning actions necessary to foster desired changes (Wright et al. 2005). At the legislative level, objectives included participating in grassroots advocacy efforts and meaningfully incorporating scientific information into policy testimony (Wright et al. 2005). These domains and skills align with the theoretical model of advocacy proposed by Earnest and colleagues, which similarly highlights the importance of relationships and policy as tools for bringing about change in communities and government (M. Earnest et al. 2023). Whether focusing on community or legislative advocacy, IM programs can overcome lack of faculty time and expertise by partnering with other leaders within their institutions. Most institutions that sponsor residency programs have community and government affairs offices. Staff in these offices understand both the policy issues affecting local community health and the advocacy skills necessary to act on them. By working with institutional government affairs teams, IM residency programs can provide effective advocacy training, even with limited resources. As recent severe cuts to funding for programs and research at universities and medical schools have shown us, the importance of legislative advocacy should not be taken lightly and should be reflected in curricula that is institution-wide.
Our study had several limitations. One limitation is that our methods did not permit assessment of temporal trends in IM advocacy curricula and, although PDs reported plans to create advocacy curricula, we do not know the extent of their plans or progress toward implementation or how subsequent social and political events may impact real-world planning and implementation. Another limitation is that we focused on formal education. Our survey questions were not intended to measure informal curricula. Finally, the survey response rate was representative of the population surveyed, but some degree of measurement error might have slightly skewed certain estimates/results. Further research is needed to determine best practices in advocacy education for learners across specialty areas and how it can be best tailored for IM learners; this also applies to assessment strategies for advocacy curriculum in IM programs, and the impact of training IM residents in population-level advocacy on patients, communities, and populations.
Overall, our results leave several unanswered questions about why some IM programs without population-level advocacy curricula are planning advocacy curricula while others are not. Among U.S.-based IM residency programs without formal advocacy curricula, few were planning to offer a population-level advocacy curriculum. Programs that were planning curricula appeared to be driven by a sense of the importance of developing population-level advocacy skills. Yet, all IM residencies surveyed who were without an advocacy curriculum faced significant barriers to implementing such curricula.
Overcoming barriers to implementing population-level advocacy curricula – including lack of expertise, faculty time, and time in existing resident curriculum – will be critical to providing effective population-level advocacy training. IM programs can address these barriers and provide effective population-level advocacy curricula by partnering with community organizations and community and government affairs staff in their home institutions. Further research is needed to understand how programs who offer population-level advocacy training now and those planning to offer it in the future are overcoming barriers to developing and teaching this much needed curricula. These findings can then be used to help support more programs to plan for and implement population-level advocacy curricula and train the future generation of health advocates to make a positive impact on detrimental social and structural determinants of health that affect their patients and the communities in which they live.
Acknowledgments
The authors thank Patricia A. Carney, PhD, MS for comments on early drafts of the manuscript.
Funding/Support
No sources of funding were reported.
Abbreviations
Accreditation Council for Graduate Medical Education (ACGME); internal medicine (IM); American Board of Internal Medicine; American College of Physicians (ACP); program directors (PDs); Association of Program Directors in Internal Medicine (APDIM); American Medical Association (AMA); graduate medical education (GME); Society of General Internal Medicine (SGIM); Leadership in Health Policy (LEAHP).
Author Contributions
JB, SD, DK, MK, and TH conceptualized and designed the study; MK coordinated data collection; JB, SD DK and BD drafted the initial manuscript; JB, SD, DK, MK, TH, BD, KM and ESW critically revised the manuscript.
Conflict of Interest Disclosures (includes financial disclosures)
The authors report no conflicts of interest.